Your Child's Hospital Journey
In-toeing
In-toeing means that when a child walks or runs, the feet turn inward instead of pointing straight ahead. It is commonly referred to as being "pigeon-toed." In-toeing usually improves as children grow. Most children with in-toeing learn to walk, run, and play sports just like children whose feet point straight ahead.
In-toeing is often first noticed by parents when a baby begins walking, but children at various ages may display in-toeing for different reasons. Three conditions can cause in-toeing:
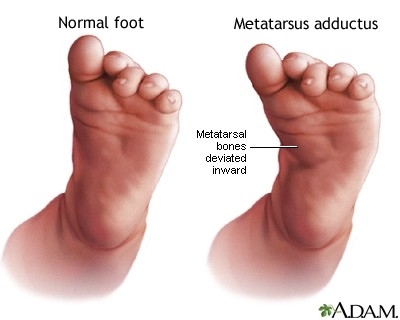
- Metatarsus adductus (the foot turns inward)
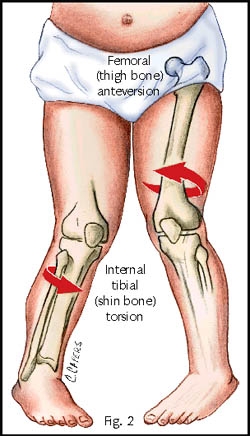
- Internal Tibial torsion (the shinbone turns inward)
- Femoral anteversion (the thighbone turns inward)
In-toeing conditions
Metatarsus Adductus
Metatarsus Adductus is when a child's feet bend inward from the middle part of the foot to the toes. Some cases may be mild and flexible, and others may be more obvious and rigid. This often results from cramped space in the womb and is evident from birth. Most will resolve spontaneously but in severe cases when the foot is stiff, stretches or advice on footwear may be necessary. Metatarsus Adductus improves by itself most of the time, usually over the first 4 to 6 months of life. Treatment in older babies and toddlers with stiff feet including casts or advice on footwear have a high rate of success. Surgery to straighten the foot is seldom required.
Internal Tibial Torsion
This occurs when the shin bone is twisted causing the foot to turn in even though the kneecaps point forwards. Many times, this is because the leg is rotated inward for the baby’s legs to fit in the mother’s womb during pregnancy. In almost all children, the tibia bone will gradually correct and untwist by itself as the walking pattern matures, but this also can take years. Splints, special shoes or exercises programmes are not necessary.
Femoral Anteversion
This is when the thighbone (femur) has a twist and turns inward. The hip can rotate inward more than usual. This is the most common cause of In-toeing. It is most evident around 4 years of age. Many kids with femoral anteversion can sit in a “W” position with their knees bent and their feet flared out behind them. Femoral anteversion spontaneously corrects in almost all children as they grow older. Usually resolving by the age of 10. This is twice as common in girls as boys and can run in families. Studies have found that special shoes or braces do not help.
W sitting:

Treatment
Normal in-toeing in a toddler requires no treatment other than observation. It can take many years for the bones to untwist as the child grows. Special shoes, braces, or chiropractic manipulation do not make the in-toeing improve any faster. If the femoral anteversion or Tibial torsion remains into secondary school and cause problems with tripping or walking, surgery may be considered to cut and rotate the bone. This is very rarely needed in otherwise normal children who have femoral anteversion / tibial torsion.
What can I do to help?
There is no evidence to suggest splints or special shoes produce any benefit, but good quality, well-fitting shoes are recommended.
Encourage your child not to W sit but to cross-leg sit instead to stretch the hips in the opposite direction, if it is comfortable for them to do so.
Out-toed activities such as ballet, horse riding, martial arts or swimming breast stroke may help an in-toeing gait.
As your child gets older, practising activities to strengthen the hip muscles, such as out-toed walking (penguin walking) or walking along a straight line (keeping feet straight) may help.
In-toeing is a normal variant of development so you do not have to restrict your child’s activities unless specifically advised to do so.